This article has been reviewed according to Science X’s editorial process
and policies. Editors have highlighted the following attributes while ensuring the content’s credibility:
fact-checked
peer-reviewed publication
trusted source
proofread
Credit: Pixabay/CC0 Public Domain
× close
Credit: Pixabay/CC0 Public Domain
Type 1 diabetes, a chronic condition affecting millions of young individuals globally, is not exclusive to childhood. As many as half of all cases are diagnosed during adulthood, and there is a need to understand the factors contributing to the development of type 1 diabetes in adults.
A new study at Karolinska Institutet now provides new insights into the development of the disease in adults. The results are presented in The Lancet Diabetes & Endocrinology.
The research, conducted at the Institute of Environmental Medicine, was based on data from more than 2.8 million individuals, and the aim was to compare the heritability of type 1 diabetes in adults and children. The findings indicate that having a first-degree relative with the condition significantly increases the risk of developing type 1 diabetes as an adult, and the risk is higher if the relative developed diabetes early. Overall, heritability is lower for type 1 diabetes in adults than children.
Yuxia Wei, Ph.D. student at the Institute of Environmental Medicine and first author, notes, “Our study provides new insights on the causes of type 1 diabetes in adults. The lower heritability in adults suggests that environmental factors play a larger role for disease development in adults than children.”
The study underscores the need for further research to identify environmental factors contributing to adult-onset type 1 diabetes. “Understanding these factors is crucial for developing targeted interventions to prevent the disease’s development,” says Sofia Carlsson, senior lecturer at the Institute of Environmental Medicine.
More information:
Yuxia Wei et al, Familial aggregation and heritability of childhood-onset and adult-onset type 1 diabetes: a Swedish register-based cohort study, The Lancet Diabetes & Endocrinology (2024). DOI: 10.1016/S2213-8587(24)00068-8
ROCHESTER — A change in federal guidelines for living organ donation opens the door for people with well-controlled Type 2 diabetes to become kidney donors.
“I think this is a very significant shift in the eligibility criteria for living kidney donation in the U.S.,” said Dr. Naim Issa, a transplant nephrologist at Mayo Clinic in Rochester, the county’s second-largest living organ donor center. “In Europe, actually, diabetes was not completely (a) contraindication to donate a kidney.”
Before the Organ Procurement and Transplantation Network updated its policies in 2022, a potential living kidney donor would be disqualified if they were diagnosed with either Type 1 or Type 2 diabetes.
“Diabetes, especially if it’s poorly controlled, can lead to complications affecting our vital organs, especially the kidneys, the eyes, the heart,” Issa said. “And diabetes, in fact, is the leading cause of kidney disease in the U.S.”
But now, people with Type 2 diabetes could become kidney donors if they meet certain critera. (Type 1 diabetes is still excluded.)
Through Mayo Clinic, a potential kidney donor would be eligible if they don’t use insulin, are not overweight, don’t have a family history of kidney disease and go through a health assessment. Right now, those donors would also need to be at least 60 years old, Issa said.
“If you’re young with Type 2 diabetes … (you’ll) have another 20, 30 years to live, and we don’t know what will happen to their kidney function and to their vital organs,” Issa said.
Additionally, potential donors between the ages of 60 and 64 would need to not be on any medications for their diabetes. But, at age 65 and older, they can be taking up to two oral medications and still be eligible, according to the Mayo Clinic guidelines.
While Issa said he only expects a “handful” of living kidney donations per year from donors who meet the Type 2 diabetes critera, he said this type of donation can be helpful in certain situations, such as when a person wants to donate a kidney to their spouse.
Dr. Naim Issa, a transplant nephrologist at Mayo Clinic in Rochester.
Contributed / Mayo Clinic
“If a wife needs a kidney, they don’t have any potential donors, instead of staying on the waiting list for five to seven years,” Issa said, “Let’s say the husband is diabetic, but very well-controlled. (He’s) lean, maybe takes one medication, older than 65 and the diabetes did not affect any of the vital organs, the heart, the kidneys or the eyes.”
The expanded critera for living kidney donation comes at a time when, Issa said, the need for kidney transplants is increasing and the wait time for kidneys from deceased donors can last years for some patients.
“People are getting older, more diabetes and more obesity causing more and more kidney disease in this country — we have more than 90,000 people waiting for a kidney transplant,” Issa said. “This is mainly to address the increasing demand fo rkidneys and provide some people with a better chance for successful transplant and, of course, improve quality of life.”
Deceased donors with diabetes have been able to donate kidneys, Issa said, if their organs weren’t substantially harmed by their diabetes.
The following is a summary of “Changes in selected hematological parameters in patients with type 1 and type 2 diabetes: a systematic review and meta-analysis,” published in the February 2024 issue of Hematology by Bambo et al.
Researchers conducted a retrospective study to uncover pooled mean differences in white and red blood cell parameters among diabetic patients, aiming to shed light on potential hematological imbalances in type 1 and type 2 diabetes mellitus.
Using appropriate entry terms, they extensively searched articles in various bibliographic databases, including PubMed, Cochrane Library, Scopus, Web of Science, PsycINFO, Embase, online archives, and university repositories. Relevant studies were identified based on eligibility criteria. Data, including author details, study characteristics, diabetes type, sample size, and hematological parameter means with SD, were extracted in Excel and analyzed in Stata 11. Pooled standardized mean difference (SMD) was determined with a random effects model, assessing heterogeneity using Higgins’ I2 statistics. Egger’s test and funnel plot analysis evaluated bias. A sensitivity analysis assessed the impact of small studies.
The results showed 39,222 articles following methodology screening, 22 articles with 14,041 participants (6,146 T2DM, 416 T1DM patients, and 7,479 HCs). Pooled SMD in TLC were 0.66, 109 for T2DM and -0.21 for T1DM. Absolute differential WBC counts in T2DM showed differences of 0.84 (neutrophils), -1.59 (eosinophils), 3.20 (basophils), 0.36 (lymphocytes), and 0.26 (monocytes). Relative differential counts in T2DM were neutrophils (1.31%), eosinophils (-0.99%), basophils (0.34%), lymphocytes (-0.19%), and monocytes (-0.64%). In T1DM, SMD of WBC 109 parameters were neutrophils (-0.10), lymphocytes (-0.69), monocytes (0.19), and basophils (-0.32). Pooled SMD in RBC parameters for T2DM were: RBC (-0.57, 106/μL), Hb (-0.73 g/dL), and HCT (-1.22%). In T1DM, RBC, Hb, and HCT were -1.23 (106/μL), -0.80 g/dL, and -0.29%, respectively.
They concluded that T2DM showed elevated white & specific cell types, while T1DM had decreased white & red blood cell parameters, highlighting diabetes’ impact on blood composition.
A Comparative Study of Semaglutide and Dapagliflozin
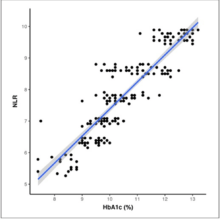
Recent advances in the field of diabetes treatment have led to a trial comparing the efficacy of two antidiabetic drugs: semaglutide and dapagliflozin. The randomized open-label trial, published in Nature, aimed to understand their effects on patients with type 2 diabetes, particularly those with severe insulin-deficient diabetes (SIDD) or severe insulin-resistant diabetes (SIRD). The study discovered that semaglutide induced a larger reduction in glycated haemoglobin (HbA1c) levels than dapagliflozin, especially in those with SIDD.
Identifying Treatment Response through Continuous Pathophysiological Variables
Interestingly, the study found no significant interaction between the drug assignment and the SIDD or SIRD subgroup. Instead, continuous pathophysiological variables such as baseline HbA1c and insulin secretion were more informative in predicting treatment response. These variables, along with body mass index, blood pressure, and insulin resistance measures, were useful in identifying patients likely to benefit most in terms of glycaemic control and cardiovascular risk factors by adding semagliflozin or dapagliflozin.
Combination Therapy: A New Approach in Type 2 Diabetes Management
Further research in Pharmacological Research evaluated the impact of combining dapagliflozin and oral semaglutide in type 2 diabetes patients. This combination therapy outperformed dapagliflozin alone by reducing glycated hemoglobin by 1.2% while improving body mass index, blood pressure, cholesterol, and glucose levels. The combination achieved 55% glycated hemoglobin near-normalization, suggesting it may induce type 2 diabetes pharmacological remission in over 50% of patients.
Implications for Clinical Practices
A related study on the combination therapy of dapagliflozin and semaglutide in PRECARE2 noted its superior efficacy in managing type 2 diabetes. The more significant reduction in HbA1c levels with the combination therapy suggests a promising approach to type 2 diabetes management, potentially changing clinical practices. This therapy offers an effective avenue for managing type 2 diabetes by significantly reducing blood sugar levels and improving other health indicators.
Cardiovascular Disease Prevention and Type 2 Diabetes Treatment
A population-based cohort study in JAMA Network Open investigated the outcomes of SGLT 2i and GLP 1RA therapy among patients with type 2 diabetes, varied by the presence or absence of NAFLD. The study found that both therapies were associated with a reduced risk of major adverse cardiovascular events in patients with type 2 diabetes, regardless of NAFLD status. Specifically, SGLT 2i therapy was associated with a reduced risk of hospitalization for heart failure, supporting current guidelines that recommend GLP 1RA as the first line of therapy for patients with type 2 diabetes and NAFLD.
Stepping Towards Precision Medicine in Diabetes
The findings of these trials highlight the potential for personalized treatment in diabetes, providing valuable insights for future clinical and scientific work in precision medicine. Continuous pathophysiological variables could be more informative in predicting treatment response than stratified subgroups, suggesting a need for a more nuanced approach in diabetes treatment. As our understanding of the disease deepens, we move closer to a future where each patient’s treatment can be tailored according to their unique physiology, bringing us one step closer to the reality of precision medicine in diabetes care.
If you are at a desk job, move around or take a small walk every two hours during the shift. Don’t go near the vending machine and slot an exercise schedule in your functional cycle, says Dr Anoop Misra, Chairman, Fortis C-DOC Hospital for Diabetes and Allied Sciences
Night owls may need to pay more attention to their lifestyle because their chronotype may increase the risk for Type-2 diabetes (Source: Getty Images)
Listen to this article Your browser does not support the audio element.
Are you a night owl? Then you are likely to have a higher risk of developing Type-2 diabetes. A recently published study from the US shows that people with “evening chronotype” or those who prefer to be active in the evening, sleep and wake up late are 19 per cent more likely to develop diabetes, even after the researchers accounted for lifestyle factors. This means that unhealthy habits may explain away a large proportion of the risk but not all of it.
“Night owls may need to pay more attention to their lifestyle because their chronotype may increase the risk for Type-2 diabetes,” say the study’s corresponding author and associate epidemiologist from Brigham and Women’s Hospital, Boston, Tianyi Huang. Chronotype refers to a person’s preferred timing of sleeping and waking up, which is partly determined by genetics, and cannot be changed easily. The study, based on data from over 63,000 women nurses, found that those who prefer to stay up and work at night are more likely to consume alcohol in higher quantities, have low-quality diet, smoke and have less physical activity.
Why does the evening chronotype increase the risk of diabetes?
You have exhausted your monthly limit of free stories.
To continue reading, simply register or sign in
Continue reading with an Indian Express Premium membership.
This premium article is free for now.
Register to read more free stories and access offers from partners.
Continue reading with an Indian Express Premium membership.
This content is exclusive for our subscribers.
Subscribe now to get unlimited access to The Indian Express exclusive and premium stories.
First, the evening chronotype is likely to develop more unhealthy lifestyle habits. “Those who go to bed late at night are much more likely to snack after dinner. When they wake up, they are unlikely to have time for exercise before heading out for work or through afternoons and evenings when they are at work,” says Dr Anoop Misra, Chairman, Fortis C-DOC Hospital for Diabetes and Allied Sciences. Those with evening chronotype are also much more likely to have an irregular sleep pattern that leads to increased glucose intolerance.
The chronotype can also impact hormones. As Dr Misra explains, “The secretion of melatonin depends on the light. Exposure to a lot of light during the night is likely to reduce melatonin secretion, which is known to regulate insulin secretion. The sleep-wake cycle also affects the cortisol levels in the body, which in turn leads to insulin resistance and obesity.”
How can I protect myself?
Dr Misra says even those with evening chronotype can reduce their risk of diabetes by following a good routine and remaining disciplined. “If a person makes time for a workout in the evening, if they do not snack at night and follow a proper routine within their functional cycle, they can have a reduced risk of diabetes.” Those with evening chronotype may also try to retrain themselves by waking up and going to bed 15 to 30 minutes earlier each day, experts say.
The US researchers found the increased risk associated with evening chronotype in nurses who worked day shifts, not those who worked overnight shifts. “When chronotype was not matched with work hours, we saw an increase in Type 2 diabetes risk. That was another very interesting finding, suggesting that more personalised work scheduling could be beneficial,” say researchers.
If you cannot avoid a night shift, Dr Misra suggests some practical ways you can remain healthy. If you are at a desk job, you should move around or take a small walk every two hours during the shift. He advises that people consume healthy snacks at night and avoid going to vending machines. People must avoid colas that may be more readily available at night than healthier beverages. Most importantly, those working night shifts should also make time for regular exercise in their routine.
“The good thing about the current study is that it has a big sample size. However, the study is based on a single questionnaire. Multiple questionnaires over a period of time would have given more details on whether the participants stuck to a particular lifestyle,” says Dr Misra.
A recent genetic study from UK scientists suggests that depression may be a direct cause of type 2 diabetes, which could support attempts to prevent the disease.
Over 500 million individuals worldwide have type 2 diabetes, which has been linked to depression through shared genetics and a causal association, according to The Guardian.
Following the study, suggestions have been made for depression to be added to the list of type 2 diabetes risk factors, along with other variables including obesity, inactivity, and a family history of the disease.
Both diseases have historically been associated with one another as people having type 2 diabetes are twice as likely to be diagnosed with depression than the general population. According to Dr Shaunak Ajinkya, Consultant, Psychiatrist, Kokilaben Dhirubhai Ambani Hospital, Mumbai, depression and type 2 diabetes have a bidirectional relationship, meaning they can influence each other and increase the risk of the other condition.
Although it was never made clear whether type 2 diabetes led to depression or vice versa, or if other factors, including obesity, were also at play. This research suggests that depression causes diabetes, rather than the other way around.
What is the relationship between depression and type 2 diabetes?
Depression can be a risk factor for type 2 diabetes because it can affect various aspects of a person’s life that are closely related to diabetes development.
Chronic stress and depression can lead to unhealthy behaviors like overeating, physical inactivity, and poor sleep, which can contribute to obesity and insulin resistance, both of which are a major risk factor for type 2 diabetes, explained Dr Sanjay Singh, General Physician, Cygnus Laxmi Hospital.
A person with a history of depression or a family history of type 2 diabetes are at higher risk. (Source: Freepik)
Additionally, depression can impact the body’s stress response system and lead to dysregulation of hormones involved in glucose metabolism, such as cortisol, insulin, and glucagon, as per Dr Ajinkya, who added that this dysregulation also contributes to the development of insulin resistance.
On the other hand, type 2 diabetes can also be a risk factor for developing depression. “The burden of managing a chronic illness, the stress associated with it, and the potential for complications can significantly affect a person’s mental health and increase the risk of depression,” Dr Ajinkya said.
What are the risk factors of developing type 2 diabetes in individuals with depression?
Assessing the risk can be done through a combination of factors, according to the experts, including:
Medical history
A person with a history of depression or a family history of type 2 diabetes are at higher risk.
Lifestyle factors
Assessing the person’s lifestyle habits, including diet, physical activity levels, and substance abuse, can help determine their risk.
Physical examination
Checking for signs of obesity or other metabolic abnormalities can provide an indication of diabetes risk.
Blood tests
Assessing fasting blood glucose levels and HbA1c (average blood glucose levels over the past few months) can help determine if a person has diabetes or is at risk of developing it.
Managing depression to reduce the risk of developing diabetes involves a multi-faceted approach. (Source: Getty Images/ Thinkstock)
If someone with depression is identified to be at risk of developing type 2 diabetes, interventions such as lifestyle modifications, regular physical activity, and mental health assessment and support may be recommended to reduce the risk and improve overall well-being.
Apart from depression, these experts say that several other risk factors can increase the likelihood of developing type 2 diabetes:
Family history of diabetes
Obesity or excess body weight, especially around the abdomen
Sedentary lifestyle
Poor diet high in sugar and unhealthy fats
High blood pressure
Age (risk increases with age)
Ethnicity (certain ethnic groups are at higher risk)
How to manage depression so that it doesn’t end up in the development of diabetes?
Managing depression to reduce the risk of developing diabetes involves a multi-faceted approach, as per the experts, such as:
Seek professional help and build a support system
Consult with a mental health expert or therapist to address and manage your depression. This may include therapy, such as cognitive-behavioral therapy (CBT), if necessary.
Seek support from friends, family, or support groups. Sharing your feelings and experiences with others who understand can help alleviate symptoms of depression.
Adopt a healthy lifestyle
Focus on regular exercise, a balanced diet, and weight management to improve insulin sensitivity and overall health. Alcohol and certain substances worsen symptoms of depression and increase the risk of developing diabetes, so it’s best to avoid their use.
Depression can be a risk factor for type 2 diabetes because it can affect various aspects of a person’s life that are closely related to diabetes development. (Source: Pixabay)
Get enough sleep
Prioritise a regular sleep schedule and aim for 7 to 9 hours of quality sleep every night. Poor sleep can worsen symptoms of depression and increase the risk of developing diabetes.
Stress management
Practice relaxation techniques such as mindfulness, yoga, or meditation to reduce stress levels. Find healthy ways to cope with stress like engaging in hobbies or activities which you enjoy.
Medication, if needed
In some cases, medication may be necessary to treat depression, and it’s essential to follow a healthcare provider’s guidance. If you are taking medication for depression, it’s important to take it as prescribed and attend regularfollow-up appointments with your healthcare provider.
If you’re at risk, maintain regular check-ups with your healthcare provider to monitor your blood sugar levels and overall health.
Remember that a collaborative approach involving mental health professionals, primary care physicians, and lifestyle modifications is crucial to manage both depression and reduce the risk of type 2 diabetes effectively.
📣 For more lifestyle news, follow us onInstagram | Twitter | Facebook and don’t miss out on the latest updates!